Families who frequently search for postpartum depression psychosis have gone through some terrifying events. Postpartum depression psychosis is rare, severe, and very time sensitive. An early check up is a way to keep babies safe, and to prevent postpartum depression psychosis (baby blues). Today’s families need to find out clearly and make fast decisions with that confidence. Coordinated, compassionate care helps ensure strong and stable results.
Treatment guidance includes CBT for Postnatal Depression: What New Moms Can Expect and insights on How Cognitive Behavioral Therapy Treats Postpartum Depression.
Understand risks when conditions escalate through When Postpartum Depression Turns Into Psychosis and read deeper with Understanding Postpartum Depression Psychosis in Mothers.
What it is and why postpartum depression psychosis develops
Postpartum psychosis is an emergency psychiatric condition following childbirth. Onset is often abrupt during the first 2 weeks. Some cases are late starters, particularly after major sleep deprivation. Delusions, hallucinations, and quickly changing mood (which may be more positive or neutral) Diminished judgment, judgment can vary hour to hour.
With past episodes or histories of bipolar spectrum disorders there is an increased risk. Severe sleep deprivation can speed the increase within a few nights. Risk factors may include changes in medications and thyroid conditions. Genetic family history provides a lot of context for monitoring, planning, and early intervention. Through a combination of agility and reaction, injury is prevented and mental wellbeing numerous times benefited for life.
Rarity and urgency have been emphasised by NIMH, RCPsych and NHS. ACOG elevates the urgency of prompt evaluation at all presentations when a diagnosis of chorioamnionitis is suspected. The third idea for families to take seriously is uncertainty, which is an invitation to early measurement. If reality testing seems unclear ask for emergency care. Waiting for clarity can be risky and can cause key steps to be delayed in protection.
Postpartum depression psychosis warning signs that are cause for alarm
Verbal directions means to teach or to give directions in an emergency. non-realistic thoughts or beliefs about the baby – represents immediate danger Another symptom of interest is abnormal agitation or grandeur. Even if the sleeplessness is coupled with rapid mood fluctuations, that implies that things are getting worse. Safety doubt needs considerable investigation the same day.
Mid-body encouragement using citations
Courage is knowing when to ask for help at the first sign of doubt.
How to tell postpartum depression psychosis apart from others
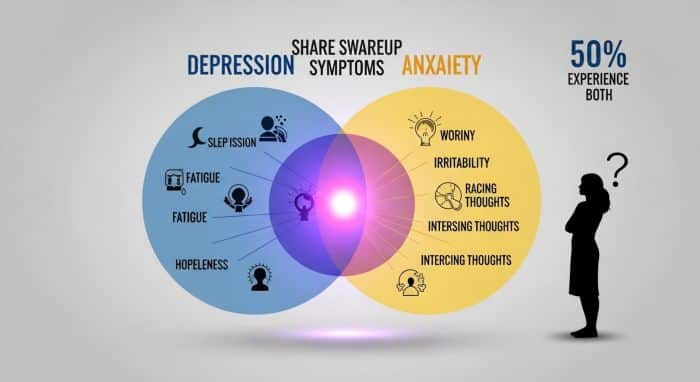
Baby blues is depression with tearfulness and lability, without delusions. Intrusive thoughts that are value-based are central to additional forms of postpartum anxiety. Postpartum depression and anxiety make pleasure less a focus and worry more a focus. Psychosis involves hallucinations, delusions and severely impaired insight. Emergency therapy to stabilize the brain and the body is needed.
The following is a shorter orientation for clinical discussions. Use it with doctors, doulas and people you trust. Review of information retained while urgent evaluation is planned. Table content must lend clarity in taking life-critical decisions Lead training of local perinatal and emergency groups.
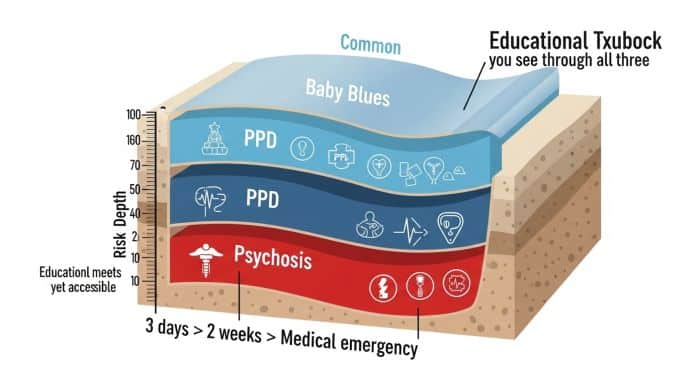
| Condition | Baby Blues | PPD / PPA | Psychosis |
|---|---|---|---|
| Onset | Days two to five | Weeks to months | Usually first two weeks |
| Core features | Tearful, overwhelmed, labile | Low mood, worry, avoidance | Delusions, hallucinations, disorganization |
| Risk level | Low; self-settling | Moderate to high | Emergency; immediate treatment |
Not every strong thought is followed by psychosis today. Intrusive thoughts are typically undesirable and ego plexing for some. Psychosis is a sign that you are obliged of an unseen vision that can’t be accepted following reassurance or confirming. If you’re not sure, assume that there is risk. Fire, police and EMS can make decisions for the safest next steps faster.
Red-Flag Alert – take immediate action if any of these are present
The boxed plan listed below can assist families to respond now with authoritative behavior: This is similar to a step-by-step guide provided with contacts and information about local resources. Save, clear or print buttons store plan for coordination purposes. This plan should be communicated to partners, family members and emergency health professionals. Keep the plan posted near a feeding or resting area.

The helplines box is a short one that should go right after the alert. Have it handy near doorway or main informal sitting area Tell relatives who are in charge of transporting or caring for the child about the numbers. Local options can be added when local pathways are substantially different Read the text of the box out loud once in calmer moments.
Educational purpose only; not a medical diagnosis; Seek licensed care.
Sequenced assessment questions clinicians perform during emergent assessments
Clinicians are distrustful of safety, speed and change of symptom. They take a sleep history and screen for medical issues. Medications and thyroid testing are permitted In many cases, baseline functioning is explained by the patients’ collateral histories. Hospital admission is for the purposes of rest, stabilization, and timely multidisciplinary care.
Mother-baby groups improve bonding and allow for safe stabilization to occur. Where possible, hospitals develop supervised contact plans with care. NICE and RCPsych advocates safety planning – individual and family level. The American College of Obstetricians and Gynecologists (ACOG) supports medical decision making by the obstetrician in collaboration with a psychiatric team. Documentation facilitates continuity between services for complex care.
You can explore detailed resources about maternal mental health starting with What Is Postpartum Depression and Why It Happens. Learn safe ways of Coping With Post Pregnancy Depression the Right Way and gain clarity through Postpartum Dep: Understanding Shortened Medical Terms.
Recognize signs from the Full List of Postpartum Depression Signs and Symptoms. Screen early using Edinburgh Postnatal: A Quick Screening Guide for New Moms.
Questionnaires for early discussion and continuing follow-up
Emphasis is given by EPDS to the pattern of depressive symptoms in the perinatal period. GAD-7 measures the type of anxiety symptom profile over the last several weeks (estimate, 4-6 weeks). Screens are used as an informational tool rather than a definitive diagnostic tool. Low scores and high impact is of course worthy professional attention. Progressive Screens to follow growth after stabilisation and discharge.
Transition and give similar quotations
You need emergency attention and emergency attention changes everything.
Therapies that assist in returning safety, sleep, and stability
Sleep restoring under supervised environment is applicable when fight explaining conditions are present. Antipsychotic/ mood stabilizer medications may be appropriate. Breastfeeding intervals are adjusted to safe, closer intervals. Risk-benefit communication respects values, culture, and realities of clinical lives. Ongoing support for lactation reduces guilt & preserves confidence.
Psychotherapy is helpful after acute symptoms have dissipated. Psychoeducation demystifies and helps to promote mutual understanding in a compassionate manner. Family therapy can help improve communications, set limits and resolve practical issues. Occupational and Social Supports – includes routines, accommodation and transport. Peer groups help eliminate isolation and make the recovery experience ‘normal’.
Some-objective improvement: Shock Electricity Can Save Lives in these cases ECT is thought when high-speed response is beneficial. Treatment selection based on severity, comorbidities and history of recurrence NIMH and APA say severe presentations are highly effective. Shared decisions are once again at the center of planning and follow-up.
Normal postpartum – interaction of postpartum depression and psychosis and mood disorders
In clinical reality, psychosis usually arises in presentations within the bipolar spectrum. The history of hypomania or mania is scrutinised carefully by clinicians. Some individuals may experience an aggravation of mood cycling while taking antidepressants alone. Mood stabilisers are thus likely to be preferred in acute phases. Long-term mood tracking helps to prevent relapse over the coming years.
The role of the partner and family during the acute and recovery stages
Have a single point person for appointment and practical management. Another adult participated in administering medications and in monitoring rest breaks that worked. Family members help monitor meals, laundry and transportation during stabilization. Messenger scripts save time and effort by removing friction during times of stress and preventing unnecessary misunderstandings. Affirmation statements keep everyone warm while they work very hard.
Aftercare, relapse prevention and planning subsequent pregnancies
Risk for relapse is high when sleep is disturbed. Address sleep: layered supports, histories, contingencies. Take your medicine as directed and go for follow-ups. Compile a written segment compliance early-warning list with specific triggers. Hand a copy of the plan to relatives who can act on your behalf.
Actively and sensitively discuss contraception and spacing with obstetric clinicians. Assess planted episode content and medication reaction frankness. Getting prepared before conception will reduce the uncertainty and reduce the delay of future response. Develop plan for postpartum monitoring prior to delivery with teams. Expectations reduce anxiety, and more people seek early help when expectations are clear.
Signs of postpartum depression psychosis in subsequent postpartum months
Some episodes begin once weaning is finished and new stressors come to the fore. Delirium-like confusion is seen in infection and severe insomnia. Restart safety plan and contact clinicians urgently. Prior recovery experience increases awareness of alertness and speed of action. commemorate the plan even when one is healthy for a long time period.
Community services that are in addition to professional services after discharge
Circadian stabilizing regimes buffer the impact of many of these to a significant degree. Timely feeding, gentle movement and bright light make all the difference. Simply be careful with caffeine and maintain proper journals in regards to stimulant chronology. Make frequent short interactions with friends and family you know and care for. Take small wins and stick to regular drug schedules every day.
Down-regulation protocols for families during stabilization and post-stabilization
Grounding techniques come in handy when there are residual anxiety or agitation waves. Remove the mandatory breathing from the body and take a gentle, long exhale. Avoid phrasing intrusive thoughts as explicit commands, and rather refer to them as “mental events.” Allow your thoughts to fail while engaging in things that you enjoy. It is also recommended to keep the sleeping environment as stimulating as possible so they can achieve more reasonable arousal control.
Action Plan – v3-compact checklist action plan daily momentum
Use this printable checklist to translate guidance into actions. Buttons remain right-aligned with a compact and space-saving header. Autosave change when hand is free caring for others. Keep the card close to feeding stations or medicine organizers. Communicate it to clinicians and supporters at each review.
Practical example scenario for families to call for emergency assistance
Parents suddenly lose sleeping habits and talking patterns become too fast. They say they are following do-as-you-see messages while making decisions and caring. The partner makes strange ideas about baby safety and feeding. Family goes into red-flag plan and contacts emergency services. Teams in a hospital are all about admitted, stabilized, sleeping and starting appropriate medicine all with great care.
Distinguishing intrusive thoughts from psychosis at stressful times
Intrusive thoughts are intra-psychic and ego-dystonic phenomena. People generally know to think of them as problematic and values-contradictory. Psychosis involves belief and loss of insight in the face of contradictory evidence. Safety deploys with real urgency given the uncertainty when the assessment must be immediately triggered. If you’re unsure how to differentiate or feel like you don’t have the time, opt for action it’s much easier to get some done than to get none done.
Understanding and respectfully engaging with culture, privacy and support networks
Growth is enhanced if plans represent cultural values and realities. Icebreakers talking directly with clinicians about language, beliefs, and decision roles. Seeking Interpreters and Cultural Brokers, as relevant and viable Memorandums of Understanding: When it comes to sensitive information, explicit agreements are warranted to confirm the privacy of the information during transfer. Communication prevents misunderstanding and offers confidence in the nature of explosive care.
Diverse documentation families should be prepared to present to urgent assessment
Keeping records of medications, dose and time last taken Keep a list of allergies, illnesses and reactions to medications Please provide contact information for family who are willing to take residence the next day. Bring baby necessities and necessities for your person that will make you feel comfortable. Duplicate copies on phones and on paper in emergency go-bags.
Tracking your progress and celebrating your victories in recovery
Keep a sleep history, sleep diary, appetite, daily activities, etc. Note decreases in restlessness, confusion and experience of suffering that week. Benefit internal accomplishments (attending events and completing tasks independently) Create a celebration and give hope and momentum to supporters Change can be non-linear but changes headed in stable directions most of the time.

More quotes comparatively to solutions and transition
For information purposes only; does not represent a diagnosis of medical conditions. Seek licensed care.
FAQs
Average prevalence of postpartum psychosis versus others?
Postpartum psychosis is very rare, unlike depression and anxiety. It is estimated that one to two cases occur per thousand births. When safety-reducing signs suddenly appear, rarity has nothing to do with urgency. Some presentations may be emergencies and require urgent evaluation. Early action reduces damage and removes long-stream behavior.
How does a clinician differentiate between psychosis and severe anxiety or depression?
Psychosis is either hallucinations, delusions or severely impaired insight. Anxiety and depression tend to allow a certain amount of reality testing. What’s important is the rapid onset of symptoms, history of travel, and sleep pattern of an individual. Clinicians check for medical causes and previous histories of mania and depression. Evidence-based Assessment determines safe choices and appropriate supports in a short time frame.
Is there a safe way to merge treatment and breastfeeding/bonding?
If you want to continue breastfeeding, there are many treatments that are safe with good planning. Medications, dosing and timing are done jointly among team members Supervised contact provides safety while diminishment continues in a compassionate manner. Intensive treatment is done so that mother and infant stay in contact with one another. Lactation support gives you time avoidance from guilt and to have upsurges of confidence for yourself.
What immediately should partners do during the acute episode?
Deploy the red-flag response and recommend emergency services at once; Be with the parent and baby until EMT arrives. In a hurry to gather medicine lists, documents and phone chargers. Have regular and supervised help from trusted family/friends. Train yourself to: be calm, not argue, observe and keep your observations short and unemotional.
The question is how to effectively reduce relapse risk after discharge in key representative family units?
Always available sleep companion in practice, changing nappies with back-up carers as needed, setting alarms and back-up carers. This involves taking medicines and going for follow-up treatments: Also, clinicians can get early alerts and connect quickly when they need to take precautions. Make emergency contacts and helplines all around the home. Encourage ongoing improvement and revision of plans after each meeting.